The HPV vaccine has been around for almost 10 years and more than 175 millions doses have been distributed in 63 countries, with several studies confirming its safety and efficacy. In spite of that, the vaccine still remains a subject of controversy. Although recommended by most scientific societies worldwide, some recent reports questioning its safety fuelled even more the debate, dividing both general public and medical community.
In this article we will analyse the existing evidence regarding the HPV vaccine, with particular focus on its efficacy and safety. In order to organise the available information, the article will be divided into the following sections:
- Getting to know HPV
- Why a vaccine? The burden of HPV-related diseases
- The three available HPV vaccines
- Vaccination schedule and timing
- Efficacy of the HPV vaccine
- Safety of the HPV vaccine
- Recent safety concerns: the chronicle of events
- Other debatable issues
- Unanswered questions…
- Conclusion
1. Getting to know HPV
 HPV (human papillomavirus) is a virus and is transmitted from person to person through skin-to-skin contact.
HPV (human papillomavirus) is a virus and is transmitted from person to person through skin-to-skin contact.
- HPV infection is extremely common, and most of the times it will be cleared by the immune system.
- Of the over 100 types of HPV, about 12 subtypes of the HPV (mostly subtypes 6 and 11) may cause genital warts (also known as condylomas). These so-called “low-risk types” can also cause a rare condition called recurrent respiratory papillomatosis, in which warts grow in the throat.
- Approximately 15 types of HPV (most commonly types 16 and 18) are related to cancer. While cervical cancer is the most common HPV-related cancer, this virus can also cause other cancers: vulvar, vaginal, anal and oropharyngeal (mouth and throat), as well as penile cancer in men.
You can read more detailed information on HPV here.
2. Why a vaccine? The burden of HPV-related diseases
 These figures will give you and idea of the magnitude of the problems caused by HPV:
These figures will give you and idea of the magnitude of the problems caused by HPV:
-Worldwide, over 500,000 new cervical cancer cases are diagnosed annually. Cervical cancer ranks as the 4th cause of female cancer in the world and is the 2nd most common female cancer in women aged 15 to 44 years (1).
In the United States, an estimated 26,000 new cancers are attributable to HPV each year, about 17,000 in women and 9,000 in men (2) .
In Europe, about 58,000 new cases of HPV-related cancers are estimated to occur every year (3).
-Regarding precancerous lesions, the estimated annual burden of high-grade precancerous lesions ranges between 280,000 and 550,000 new cases per year in Europe (4).
-In addition to cancers and precancerous lesions, the problem of genital warts should also be taken into consideration. Genital warts are very common: 1 out of 10 persons will have condylomas at some point in their lives (the frequency varies according to different countries between 0,3 and 12 %) (5). About 800,000 new annual genital warts cases are estimated to occur in women and men in Europe (4). Although not life-threatening, the costs derived from their treatment and their psychological burden should not be neglected.
3. The three available HPV vaccines
 From 2006, 2 vaccines have been available: One bivalent (Cervarix®), directed against HPV types 16 and 18, responsible for about 70% of cervical cancers and other HPV-associated cancers; the other quadrivalent (Gardasil® of Silgard® in different countries) containing 4 HPV types:16 and 18, together with HPV 6 and 11 which are responsible for more than 90% of genital warts.
From 2006, 2 vaccines have been available: One bivalent (Cervarix®), directed against HPV types 16 and 18, responsible for about 70% of cervical cancers and other HPV-associated cancers; the other quadrivalent (Gardasil® of Silgard® in different countries) containing 4 HPV types:16 and 18, together with HPV 6 and 11 which are responsible for more than 90% of genital warts.
In December 2014, the American Food and Drug Administration (FDA) approved a nine-valent vaccine, Gardasil 9® (6), which, besides the 4 strains contained in Gardasil (i.e., 6,11,16,18), includes types 31, 33, 45, 52, and 58, responsible for an additional 20% of HPV-related cancers (4). Gardasil 9 has also been recently approved for commercialisation in Europe (7).
4. Vaccination schedule and timing
- Vaccines are given as a 3-dose series, Gardasil at 0, 2 and 6 months, Cervarix at 0, 1 and 6 months (8).
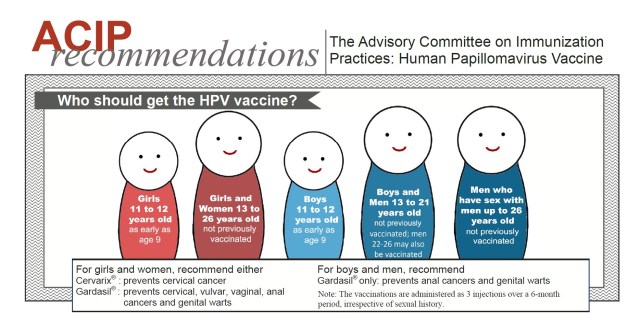
- In the States, The Advisory Committee on Immunization Practices (ACIP) and the American College of Obstetrician and Gynecologists (ACOG) recommend that girls be routinely vaccinated at age 11 or 12 years.
- Since 2010 boys have been included in the vaccination schedule in the USA, with the same schedule as girls.
- If not vaccinated when they were younger, girls/young women and boys/young men should be vaccinated through age 26 (9).
- Vaccine may be given starting at age 9 years (9, 10).
- A reduced, 2-dose schedule is recommended by the World Health Organization (WHO) for those aged 9-13 years; this schedule is not recommended by the ACIP but it has been adopted by many countries.

- Earlier vaccination (before age 14) results in higher immune response. Another argument in favor of early vaccination is the fact that vaccines are more effective before the onset of sexual activity (8).
- Vaccination is recommended regardless of sexual activity or known HPV infection. Although vaccines seem to be less effective in sexually active people, some benefit is expected to be attained since exposure to all types of HPV included in the vaccines is very unlikely. Testing for HPV is NOT recommended before vaccination.
- The vaccines are prophylactic, that is, they do not prevent progression of existing infection to disease or treat existing disease. (2)
- The HPV vaccine is covered by most private health insurance and government insurance programs worldwide. Vaccinations schedules may vary in different countries.
- There seems to be additional protection by the vaccine in women through age 45, as showed by certain studies (11). However, there is no recommendation for vaccination in individuals aged 26 to 45.
- The same schedule applies for Gardasil 9 (0, 2 and 6 months). Revaccination with the nine-valent vaccine is not recommended in persons who previously completed the three-dose series with the bivalent or or quadrivalent HPV vaccine (8).
5. Efficacy of the HPV vaccine
 The ultimate goal of the HPV vaccine is to reduce the incidence of HPV-related cancers. For obvious ethical reasons, the endpoint set to evaluate the HPV vaccine efficacy in different studies was precancerous lesions, namely CIN 2 and 3 (high risk lesions of the cervix, with potential to evolve to cancer). Other efficacy endpoints evaluated were incidence of HPV infection and incidence of condylomas.
The ultimate goal of the HPV vaccine is to reduce the incidence of HPV-related cancers. For obvious ethical reasons, the endpoint set to evaluate the HPV vaccine efficacy in different studies was precancerous lesions, namely CIN 2 and 3 (high risk lesions of the cervix, with potential to evolve to cancer). Other efficacy endpoints evaluated were incidence of HPV infection and incidence of condylomas.
Studies conducted before licensure showed that both vaccines achieved a high level of protection: 98-100% for the HPV types included in the vaccine in a naive population (that is, women who did not have HPV 16 or 18 at the time of vaccination), although the protection against precancerous lesions was 30-40% in the total vaccinated cohort (which included women who did not finish their immunization plan, or that were already infected with the virus before vaccination) (12, 13, 14, 15). There was also cross-protection for other types of HPV (i.e., HPV 45 and 31), which was more intense with Cervarix (16).
 The impact of vaccination on the general population has also been analysed in some studies. Australia was the first country to introduce an organised HPV vaccination program, achieving one of the world’s highest vaccination compliance rates. Since 2007, when the National HPV vaccination program started with the quadrivalent vaccine, HPV infections from the types included in the vaccine decreased from 29% to 7% (17); a 93% reduction in the diagnosis of genital warts was also observed (18). Moreover, other recent studies showed an almost 50% reduction of high-grade cervical precancerous lesions in women who had received all required doses of the vaccine (19).
The impact of vaccination on the general population has also been analysed in some studies. Australia was the first country to introduce an organised HPV vaccination program, achieving one of the world’s highest vaccination compliance rates. Since 2007, when the National HPV vaccination program started with the quadrivalent vaccine, HPV infections from the types included in the vaccine decreased from 29% to 7% (17); a 93% reduction in the diagnosis of genital warts was also observed (18). Moreover, other recent studies showed an almost 50% reduction of high-grade cervical precancerous lesions in women who had received all required doses of the vaccine (19).
Denmark also counts with an organised vaccination program. Six years after licensure of the quadrivalent HPV vaccine, a reduction of cervical precancerous lesions was observed, which was 80% in younger patients (20).
Recently, a study was conducted to evaluate the efficacy of the nine-valent vaccine. Gardasil 9 prevented 97% of high-grade precancerous lesions of the cervix, vulva, and vagina caused by the five new high-risk HPV types (HPV31/33/45/52/58) (21). The nine-valent vaccine also generated immune responses to HPV6/11/16/18 that were as good as or better than those generated by the quadrivalent vaccine. (4, 22)
6. Safety of the HPV vaccine
Many studies have evaluated HPV vaccine safety, both before their commercialisation and post-release, which demonstrated no differences in side effects as compared to control groups, irrespective of age and ethnicity (23).
 According to the CDC, the most commonly reported side effects of the vaccines are:
According to the CDC, the most commonly reported side effects of the vaccines are:
- Pain, redness, or swelling in the arm where the shot was given
- Fever
- Headache or feeling tired
- Nausea
- Muscle or joint pain
Fainting (also known as syncope) and related symptoms (such as jerking movements) is not uncommon (24), especially in teenagers. For that reason, it is recommended that people receiving the HPV vaccine sit or lie down during vaccination, and remain seated for 15 minutes after the shot. (23)
Considering the target age of vaccination (which includes women in reproductive age), pregnancy outcomes received special attention. No increase in miscarriage rates has been reported for either of the vaccines (25). In addition, pregnant women that were recorded and observed in registrative trials did not have increased rate of congenital abnormalities (26, 27, 24).
Studies have also demonstrated efficacy and safety of the vaccines in men, both in heterosexual and men who have sex with men (28).
Serious side effects are very rare (less than 0.5%) (29), the most common being persistent headache, hypertension, gastroenteritis, bronchospasm and anaphylaxis. Their reported incidence is similar to that of other compulsory vaccines types (30).
 Certain side effects have been a matter of concern since the introduction of the vaccine, namely autoimmune diseases (AD) (i.e., hypothyroidism, rheumatoid arthritis, Behçet’s syndrome, Raynaud’s disease, type 1 diabetes, and vitiligo), neurological disorders (such as epilepsy, paralysis, Guillain–Barré syndrome, central demyelination, and multiple sclerosis) and venous thromboembolism (a blood clot that plugs a vein). It should be mentioned that ADs are not rare in adolescents and young adults, particularly in women. Therefore, it is a real challenge to distinguish causal from temporal association. A recent study gathered the results of 9 large studies (of which one was an analysis of 42 trials together, or metanalysis) in order to investigate severe adverse reactions after the HPV vaccine. None of the included studies found evidence of increased risk of autoimmune disease, neurological disorder, or venous thromboembolism (31).
Certain side effects have been a matter of concern since the introduction of the vaccine, namely autoimmune diseases (AD) (i.e., hypothyroidism, rheumatoid arthritis, Behçet’s syndrome, Raynaud’s disease, type 1 diabetes, and vitiligo), neurological disorders (such as epilepsy, paralysis, Guillain–Barré syndrome, central demyelination, and multiple sclerosis) and venous thromboembolism (a blood clot that plugs a vein). It should be mentioned that ADs are not rare in adolescents and young adults, particularly in women. Therefore, it is a real challenge to distinguish causal from temporal association. A recent study gathered the results of 9 large studies (of which one was an analysis of 42 trials together, or metanalysis) in order to investigate severe adverse reactions after the HPV vaccine. None of the included studies found evidence of increased risk of autoimmune disease, neurological disorder, or venous thromboembolism (31).
The Global Advisory Committee on Vaccine Safety (GACVS), established by the World Health Organization (WHO) provides independent, scientifically rigorous advice on vaccine-safety issues. In December 2013, the committee reviewed different topics and considered all available evidence on the safety of HPV vaccines, and concluded that both commercially available vaccines are safe (32). Likewise, the International Federation of Gynecology and Obstetrics (FIGO) Gynecologic Oncologic Committee and Subcommittee for Cervical Cancer Prevention support the continued administration of the HPV vaccines in appropriate populations (33).
7. Recent safety concerns: the chronicle of events
 Although some isolated cases of side effects had been described in UK and Australia (34), Japan was the first country reporting on several girls suffering from severe pain and disability; these cases were heavily publicised in newspapers, TV news and social media, but they also alarmed the medical community. Japanese physicians published later on a series of 44 girls who were diagnosed with complex regional pain syndrome (CRPS) (35). Due to these concerns, in June 2013 the Japanese Ministry of Health, Labour, and Welfare (MHLW) decided to suspend its active recommendation of HPV vaccination. This decision created intense debate among scientists and general public, which continues until nowadays (34).
Although some isolated cases of side effects had been described in UK and Australia (34), Japan was the first country reporting on several girls suffering from severe pain and disability; these cases were heavily publicised in newspapers, TV news and social media, but they also alarmed the medical community. Japanese physicians published later on a series of 44 girls who were diagnosed with complex regional pain syndrome (CRPS) (35). Due to these concerns, in June 2013 the Japanese Ministry of Health, Labour, and Welfare (MHLW) decided to suspend its active recommendation of HPV vaccination. This decision created intense debate among scientists and general public, which continues until nowadays (34).
In March 2015, Denmark‘s TV channel TV2 aired a documentary entitled The Vaccinated Girls – Sick and Betrayed. The journalists gathered about 60 girls from all over Denmark who became sick shortly after receiving the HPV vaccine. Among the doctors interviewed is Louise Brinth, who examined approximately 80 girls with similar symptoms potentially caused by the HPV vaccine. Dr. Brinth noted that the girls experience symptoms such as dizziness, passing out, and severe headaches. She said, “They have abdominal pain and nausea. They have weird muscle movements they cannot control. And they’re very tired… We see a pattern that screams to heaven, and that should be examined by some solid research.”
 In April 2015, Dr. Brinth reported in a scientific journal on 53 patients complaining of orthostatic intolerance, severe headache, excessive fatigue, cognitive dysfunction, gastrointestinal discomfort and widespread pain. Most of them were diagnosed with a rare syndrome known as postural orthostatic tachycardia syndrome (POTS), and all of them were in close temporal association with the HPV vaccine (36a, 36b).
In April 2015, Dr. Brinth reported in a scientific journal on 53 patients complaining of orthostatic intolerance, severe headache, excessive fatigue, cognitive dysfunction, gastrointestinal discomfort and widespread pain. Most of them were diagnosed with a rare syndrome known as postural orthostatic tachycardia syndrome (POTS), and all of them were in close temporal association with the HPV vaccine (36a, 36b).
Denmark’s documentary has had a huge impact worldwide, both in the general public and the medical community. A closed Facebook page set up for suspected victims of adverse reactions to Gardasil in Denmark tripled its -careful verified- members; similar Facebook groups were created in other countries.
At the request of Denmark, The European Medicines Agency (EMA) is currently conducting a safety review of HPV vaccines. However, the agency emphasizes that this review “does not question that the benefits of HPV vaccines outweigh their risks.”The agency also notes that while the review is being carried out, no change in the use of these products is recommended. See the EMA’s review conclusions here.
 In May 2015, UK’s newspaper The Independent published an article entitled: Thousands of teenage girls report feeling seriously ill after routine school cancer vaccination. The article focuses on the story of Emily Ryalls, 17, who started feeling intense pains and difficulty breathing soon after receiving the HPV vaccine.
In May 2015, UK’s newspaper The Independent published an article entitled: Thousands of teenage girls report feeling seriously ill after routine school cancer vaccination. The article focuses on the story of Emily Ryalls, 17, who started feeling intense pains and difficulty breathing soon after receiving the HPV vaccine.
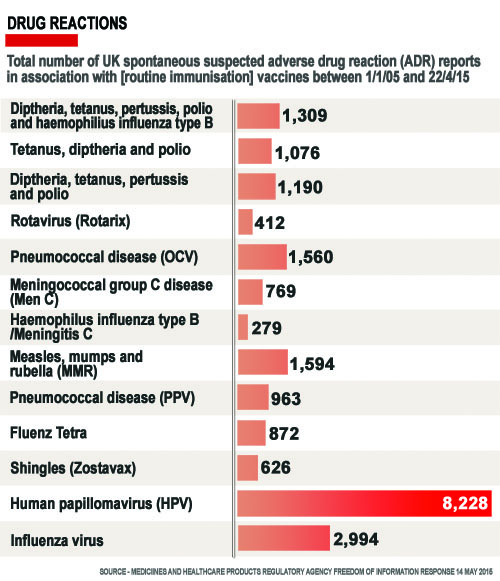
Mrs Ryalls reported Emily’s symptoms to the Medicines and Healthcare Products Regulatory Agency (MHRA), and she was not alone: adverse reactions after HPV vaccination numbered 8,228, of which 2,587 were classified as “serious”; that’s substantially more that those reported with other compulsory vaccines (see graph). The MHRA, though, said it had no concerns on the numbers of adverse reactions related to the HPV vaccine and that the “expected benefits in preventing illness and death from HPV infection outweigh the known risks”.
Emily’s mother, together with other 80 families in similar situation across the UK have formed the Association for HPV Vaccine Injured Daughters (AHVID).
As stated by the newspaper “This article created significant debate among medical professionals, journalists and members of the public…”.
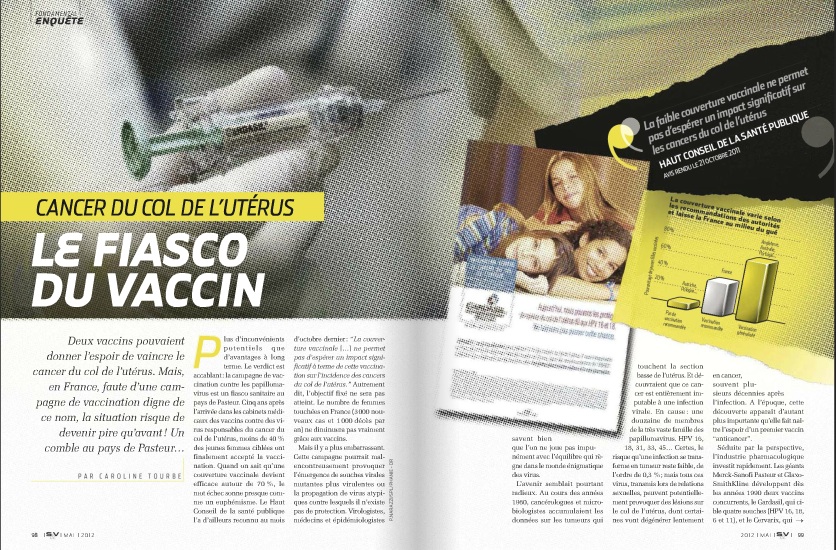
 In France, the National Security Agency of Medicines and Health Products (ANSM) just published (September 2015) the results of the follow-up of more than 2 million girls aged 13-16 years, vaccinated between 2008 and 2013 to evaluate the occurrence of side effects, mainly autoimmune diseases. When analysed all the diseases together, their results showed no overall increased risk of occurrence of serious events. However, when each disease was analysed individually, a four-fold increase in the occurrence of Guillain Barre syndrome was observed. The study also found an increased risk of Inflammatory Bowel disease, but the association was weak.
In France, the National Security Agency of Medicines and Health Products (ANSM) just published (September 2015) the results of the follow-up of more than 2 million girls aged 13-16 years, vaccinated between 2008 and 2013 to evaluate the occurrence of side effects, mainly autoimmune diseases. When analysed all the diseases together, their results showed no overall increased risk of occurrence of serious events. However, when each disease was analysed individually, a four-fold increase in the occurrence of Guillain Barre syndrome was observed. The study also found an increased risk of Inflammatory Bowel disease, but the association was weak.
The authors conclude: “…the results of the study… prove reassuring regarding the risk of autoimmune disease associated with the HPV vaccines. The expected benefits of this vaccination in terms of public health are far greater than the eventual risks the girls may be exposed to” (37). In spite of these “reassuring” results, the vaccination rate in France continue to be low (less than 30%).
 In September 2015, another report provided details on 45 individuals from 13 countries who developed a chronic ailment soon after receiving the HPV vaccine. “A disabling syndrome of chronic neuropathic pain, vexing fatigue, and profound autonomic dysfunction may appear after HPV vaccination,” say the authors, headed by Manuel Martínez-Lavín, MD, a specialist in chronic pain conditions from Mexico City. After a mean period of 4 years following HPV vaccination, 93% of individuals “continue to have incapacitating symptoms and remain unable to attend school or work,” write the authors (38).
In September 2015, another report provided details on 45 individuals from 13 countries who developed a chronic ailment soon after receiving the HPV vaccine. “A disabling syndrome of chronic neuropathic pain, vexing fatigue, and profound autonomic dysfunction may appear after HPV vaccination,” say the authors, headed by Manuel Martínez-Lavín, MD, a specialist in chronic pain conditions from Mexico City. After a mean period of 4 years following HPV vaccination, 93% of individuals “continue to have incapacitating symptoms and remain unable to attend school or work,” write the authors (38).
POTS after HPV vaccination has also been reported in the United States. Dr. Blitshteyn, a neurologist from New York, described six patients who developed POTS between 6 days and 2 months after HPV vaccination. All patients reported improvement over 3 years, but residual symptoms persisted (39).
The US Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) emphasised that controlled clinical trials in tens of thousands of individuals plus postlicensure monitoring of millions of individuals have found no causal association between HPV vaccination and atypical pain syndromes or autonomic dysfunction.
 Dr. Diane Harper, an american obstetrician & gynecologist, is one of the HPV experts called in to design the clinical trials of Gardasil and Cervarix. Although initially in favour of the vaccine, in recent years she has questioned Gardasil safety. She stated that “Gardasil has been associated with at least as many serious adverse events as there are deaths from cervical cancer developing each year”. Moreover, in an article published in December 2009 she concluded that, given the various limitations and risks of the vaccines, the benefits and risks of HPV vaccination must be weighed with the benefits and risks of HPV screening (Pap smears) to reduce cervical cancer in a cost-effective manner (40).
Dr. Diane Harper, an american obstetrician & gynecologist, is one of the HPV experts called in to design the clinical trials of Gardasil and Cervarix. Although initially in favour of the vaccine, in recent years she has questioned Gardasil safety. She stated that “Gardasil has been associated with at least as many serious adverse events as there are deaths from cervical cancer developing each year”. Moreover, in an article published in December 2009 she concluded that, given the various limitations and risks of the vaccines, the benefits and risks of HPV vaccination must be weighed with the benefits and risks of HPV screening (Pap smears) to reduce cervical cancer in a cost-effective manner (40).
Dr. Harper does not support mandatory HPV vaccination for schoolchildren, because she believes that the duration of protection may be too short (see below). She has also criticised the short period of time vaccines were tried before its licensure, and the misleading publicity carried out by the pharmaceutical companies. Learn more here.
8. Other debatable issues
Vaccination in boys

The rationale of vaccinating boys is to reduce the transmission of the HPV virus to women and to protect them against oral and anal cancers (41). Since these cancers are very rare, it has been questioned by some scientists whether is it worth to expose millions of boys to potential vaccine side effects in order to protect girls, or to prevent a so rare type of cancer (responsible for just 300 deaths in the USA); whether the benefit outweighs the risk and if men vaccination is cost effective. While countries such as Australia and the USA include boys in their vaccine recommendations, other countries (i.e., UK and France) have not yet adopted this measure.
Men who have sex with men are a special category, since they are at higher risk of anal cancer. Thus, some experts believe these men (and not every boy) should be offered the vaccine. However, this measure may be difficult to implement: in order get covered by their insurance or social security, young men may be required to declare their sexual preferences.
Immunogenicity of Gardasil vs. Cervarix
 Immunogenicity means the ability of the vaccine to provoke an immune response; in other words, the “strength” of the vaccine.
Immunogenicity means the ability of the vaccine to provoke an immune response; in other words, the “strength” of the vaccine.
Most countries adopted vaccination with Gardasil instead of Cervarix assuming equal protection for cancer, with the “bonus” protection against genital warts. But is it really like this?
Several studies have demonstrated that Cervarix elicits stronger and longer-lasting immune response than Gardasil (42, 43).
These laboratory findings have also been confirmed by some clinical studies: Over the years, the efficacy of the Cervarix to protect vaccinated women from precancerous lesions (total vaccinated cohort-naive) was 93%, while Gardasil’s dropped to 43% (44)
Age of vaccination
 This subject has also raised intense debate and concern. As stated above, immune response provoked by the vaccines may be of limited duration, especially for Gardasil. This can be a serious limitation of the vaccine because, as Dr. Harper noted “… if the HPV vaccine does not last for at least 15 years, no cancers will ever be prevented; women will just get the cancers at a later time in life after the vaccine has worn off“.
This subject has also raised intense debate and concern. As stated above, immune response provoked by the vaccines may be of limited duration, especially for Gardasil. This can be a serious limitation of the vaccine because, as Dr. Harper noted “… if the HPV vaccine does not last for at least 15 years, no cancers will ever be prevented; women will just get the cancers at a later time in life after the vaccine has worn off“.
If this short protection span is confirmed by clinical studies, a boost dose would solve this limitation. However, this would increase considerably the cost of the vaccine; moreover, women who don’t comply with this recommendation will become unprotected over time.
Increase of promiscuity?
Many people feared that the the HPV vaccine would lead girls to promiscuous behavior. This was actually investigated by some studies, and have proved not to be true: no increase in sexually transmitted diseases was observed among vaccinated girls (45), showing that vaccination is unlikely to promote unsafe sexual activity.
9. Unanswered questions…
 Will the HPV vaccine reduce cervical cancer deaths in real-world conditions?
Will the HPV vaccine reduce cervical cancer deaths in real-world conditions?- In light of the latest publications, should vaccination programs be halted until the situations is clarified?
- Due to these latest concerns, will more women opt for no vaccination, missing the opportunity to be protected against cancer?
- Since the syndromes potentially related to vaccines are difficult to diagnose, is it possible that they have been underreported in the past? Could they possibly become over reported in the future?
- Will the vaccine create a false sense of full protection against cervical cancer, resulting in less women attending screening programs?
- Will the vaccine lead to a reduction of the HPV types included in the vaccine, but to an increase of those not included in the vaccine?
10. Conclusion
 It is indeed exciting to have a vaccine that protects against cancer. After seeing women dying from cervical cancer, I truly wish that cervical cancer will be eradicated in the future. But we MUST be sure that we don’t create more harm than good in the process.
It is indeed exciting to have a vaccine that protects against cancer. After seeing women dying from cervical cancer, I truly wish that cervical cancer will be eradicated in the future. But we MUST be sure that we don’t create more harm than good in the process.
 I am in favor of vaccines. Vaccines have done a lot of good to humanity (just imagine if we would still have small pox, or poliomyelitis…). It is true that every single medical practice may come with side effects, and this include vaccines. But we MUST know exactly what are the vaccine risks, and whether the benefits outweigh the risks.
I am in favor of vaccines. Vaccines have done a lot of good to humanity (just imagine if we would still have small pox, or poliomyelitis…). It is true that every single medical practice may come with side effects, and this include vaccines. But we MUST know exactly what are the vaccine risks, and whether the benefits outweigh the risks.
I firmly believe that governments, scientific societies and pharmaceutical companies MUST do an effort to inform people in a responsible and honest manner, so that all of us -young people, parents and physicians- continue to believe in good science, and vaccines don’t lose their credibility.
It will take 10 to 20 years to figure out the true benefit of the HPV vaccine. In the meantime, keep in mind that Pap tests never killed anyone, on the contrary, they have saved millions of lives. Therefore, don’t forget your Pap smear!
Read on the latest events related to the HPV vaccine here.
References
- International Agency for Research on Cancer, World Health Organization. Globocan 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012
- CDC Grand Rounds: Reducing the Burden of HPV-Associated Cancer and Disease. Morbidity and Mortality Weekly Report (MMWR) January 31, 2014 / 63(04);69-72
- Human Papillomavirus and Related Diseases Report. hpvcentre.net March 20th, 2015
- Hartwig S, et al: Estimation of the epidemiological burden of HPV-related anogenital cancers, precancerous lesions, and genital warts in women and men in Europe: Potential additional benefit of a nine-valent second generation HPV vaccine compared to first generation HPV vaccines. Papillomavirus Research, In Press (Available online 16 June 2015)
- Patel H, et al: Systematic review of the incidence and prevalence of genital warts. BMC Infectious Diseases 2013, 13:39
- “FDA approves Gardasil 9 for prevention of certain cancers caused by five additional types of HPV” (press release). 10 December 2014.
- “Gardasil® 9: new HPV vaccine approved in the European Union. The European Commission grants marketing authorisation for the first 9-valent HPV vaccine” (press release) Sanofi Pasteur MSD, June 17, 2015.
- Human Papillomavirus Vaccination. The American College of Obstetricians and Gynecologists, Committee Opinion Number 641, September 2015
- Recommendations on the Use of Quadrivalent Human Papillomavirus Vaccine in Males — Advisory Committee on Immunization Practices (ACIP), 2011. Morbidity and Mortality Weekly Report (MMWR), December 23, 2011 / 60(50);1705-1708
- Markowitz L, et al: Quadrivalent Human Papillomavirus Vaccine Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity and Mortality Weekly Report (MMWR), March 23, 2007 / 56(RR02);1-24
- Castellsagué X, et al: HPV vaccination against cervical cancer in women above 25 years of age: key considerations and current perspectives. Gynecologic Oncology 115 (2009) S15–S23
- Villa L, et al: Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: a randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol 2005; 6: 271–78
- The FUTURE II Study Group: Quadrivalent Vaccine against Human Papillomavirus to Prevent High-Grade Cervical Lesions. N Engl J Med 2007;356:1915-27
- Paavonen J, et al: Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet, Vol 374, No. 9686, p301–314, 25 July 2009
- Lehtinen M, et al: Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol, Vol 13, No. 1, p89–99, January 2012
- Harper D: Prophylactic human papillomavirus vaccines to prevent cervical cancer: review of the Phase II and III trials. Therapy 2008, 5 (3), 313-324
- Tabrizi SN, et al: Fall in human papillomavirus prevalence following a national vaccination program. J Infect Dis. 2012; 206(11):1645-1651
- Mariani L, et al: Early direct and indirect impact of quadrivalent HPV (4HPV) vaccine on genital warts: a systematic review. Adv Ther, 32 (2015), pp. 10–30
- Crowe E, et al: Effectiveness of quadrivalent human papillomavirus vaccine for the prevention of cervical abnormalities: case-control study nested within a population based screening programme in Australia. BMJ 2014;348:g1458
- Baldur-Felskov B, et at: early impact of Human Papillomavirus Vaccination on cervical Neoplasia—Nationwide Follow-up ofYoung Danish Women. J Natl Cancer Inst (2014) 106(3): djt460 doi:10.1093/jnci/djt460
- Joura E, et al: A 9-Valent HPV Vaccine against Infection and Intraepithelial Neoplasia in Women. N Engl J Med 2015; 372:711-723
- Petrosky E, et al: Use of 9-Valent Human Papillomavirus (HPV) Vaccine: Updated HPV Vaccination Recommendations of the Advisory Committee on Immunization Practices. Morbidity and Mortality Weekly Report (MMWR), March 27, 2015 / 64(11);300-304
- Center for Disease Control and Prevention. Human Papillomavirus (HPV) Vaccine Safety. Updated September 28, 2015
- Slade BA, et al: Postlicensure safety surveillance for quadrivalent human papillomavirus recombinant vaccine. JAMA, 2009;302(7):750–757
- Wacholder S, et al: Risk of miscarriage with bivalent vaccine against human papillomavirus (HPV) types 16 and 18: pooled analysis of two randomised controlled trials. BMJ 2010;340:c712
- Garland SM, et al: Pregnancy and infant outcomes in the clinical trials of a human papillomavirus type 6/11/16/18 vaccine: a combined analysis of five randomized controlled trials. Obstet Gynecol 2009;114(6):1179–1188
- Dana A, Buchanan KM, Goss MA, et al. Pregnancy outcomes from the pregnancy registry of a human papillomavirus type 6/11/16/18 vaccine. Obstet Gynecol. 2009;114(6):1170–1178
- Moscicki A, et al: HPV in men: an update. J Low Genit Tract Dis. 2011 Jul; 15(3): 231–234
- Gonçalves AK, et al: Safety, tolerability and side effects of human papillomavirus vaccines: a systematic quantitative review. Braz J Infect Dis, Vol 18, Issue 6, Nov–Dec 2014, Pages 651–659
- Lu B, et al: Efficacy and safety of prophylactic vaccines against cervical HPV infection and diseases among women: a systematic review and meta-analysis. BMC Infect Dis. 2011;11:13
- De Vincenzo R, et al: Long-term efficacy and safety of human papillomavirus vaccination. International Journal of Women’s Health 2014:6 999–1010
- World Health Organization. Global Advisory Committee on Vaccine Safety, 11–12 December 2013: Human papillomavirus vaccines safety (HPV). Wkly Epidemiol Rec. 2014;89(7):58–60
- Denny L: Safety of HPV vaccination: a FIGO statement. Int J Gynaecol Obstet. 2013;123(3):187–188
- Wilson R, et al: HPV Vaccination in Japan. The Continuing Debate and Global Impacts. A Report of the CSIS Global Health Policy Center. April 2015
- Kinoshita T, et al: Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine. Intern Med 53: 2185-2200, 2014
- a: Brinth L, et al: Suspected side effects to the quadrivalent human papilloma vaccine. Dan Med J 2015;62(4):A5064 b: Brinth L, et al: Orthostatic intolerance and postural tachycardia syndrome as suspected adverse effects of vaccination against human papilloma virus. Vaccine, 2015 May 21;33(22):2602-5
- Vaccination contre les infections à HPV et risque de maladies auto-immunes : une étude Cnamts/ANSM rassurante – Point d’information 13/09/2015
- Martínez-Lavín M, et: HPV vaccination syndrome. A questionnaire-based study. Clinical Rheumatology pp 1-3. Online 10 September 2015
- Blitshteyn S. Postural tachycardia syndrome following human papillomavirus vaccination. Eur J Neurol, Vol 21, 1, 135–139, 2014
- Harper, D: Current prophylactic HPV vaccines and gynecologic premalignancies. Current Opinion in Obstetrics and Gynecology 2009, 21:457–464
- Giuliano A, et al: Efficacy of Quadrivalent HPV Vaccine against HPV Infection and Disease in Males. N Engl J Med 2011;364:401-11
- Einstein M, et al: Comparative immunogenicity and safety of human papillomavirus (HPV)- 16/18 vaccine and HPV-6/11/16/18 vaccine: follow-up from months 12-24 in a Phase III randomized study of healthy women aged 18-45 years. Human Vaccines, vol. 7, no. 12, pp. 1343–1358, 2011
- Barzon L, et al: Neutralizing and cross-neutralizing antibody titres induced by bivalent and quadrivalent human papillomavirus vaccines in the target population of organized vaccination programmes. Vaccine, vol. 32, no. 41, pp. 5357–5362, 2014
- Di Mario S, et al: Are the Two Human Papillomavirus Vaccines Really Similar? A Systematic Review of Available Evidence: Efficacy of the Two Vaccines against HPV. Journal of Immunology Research, Volume 2015 (2015), Article ID 435141, 13 pages
- Jena A, et al: Incidence of Sexually Transmitted Infections After Human Papillomavirus Vaccination Among Adolescent Females. JAMA Intern Med. 2015;175(4):617-623
Photo Credits
Intro: Getty images; 1: curecancer.org; 2: m2.behance.net; 3: (collage) wikimedia commons; 4: cityofchicago.org; nkytribune.com; 5: english.cri.cn; hpv.health.gov.au; 6: marketingmag.ca; scontent.cdninstagram.com; 7: Japan: wikimedia commons; Denmark: vaccineimpact.com; UK: independent.co.uk; France: science-et-vie.com; POTS: pinterest.com; Harper: initiativecitoyenne.be; 8: bphc.org; migueljara.files.wordpress.com; lh3.googleusercontent.com; 9: healthvermont.gov; 10: compasscayman.com; i.dailymail.co.uk

 Egg donation may be considered in the following situations:
Egg donation may be considered in the following situations: 1) Anonymous, voluntary donors: According to the Greek law, candidate egg donors are covered by anonymity and are required to sign a specific consent for the donation of their genetic material. In order to accept a woman into an egg donation program she should meet the following requirements:
1) Anonymous, voluntary donors: According to the Greek law, candidate egg donors are covered by anonymity and are required to sign a specific consent for the donation of their genetic material. In order to accept a woman into an egg donation program she should meet the following requirements:







































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}