Το εμβόλιο κατά του ιού του ανθρωπίνου θηλώματος (HPV) κυκλοφορεί εδώ και σχεδόν 10 χρόνια και πάνω από 175 εκατομμύρια δόσεις έχουν χορηγηθεί σε 63 διαφορετικές χώρες. Παρόλα αυτά, το εμβόλιο παραμένει αμφιλεγόμενο. Ενώ συνιστάται από τις περισσότερες επιστημονικές εταιρείες παγκοσμίως, ορισμένες πρόσφατες μελέτες που αμφισβητούν την ασφάλεια του, τροφοδότησαν ακόμη περισσότερο τη διαμάχη, και έχουν διχάζει τόσο το ευρύτερο κοινό όσο και την ιατρική κοινότητα.
Σε αυτό το άρθρο θα αναλύσουμε τα δεδομένα σχετικά με το εμβόλιο κατά του HPV, με ιδιαίτερη έμφαση στην αποτελεσματικότητα και την ασφάλειά του. Για να οργανώσουμε τις διαθέσιμες πληροφορίες, το άρθρο θα χωρίζεται στις ακόλουθες ενότητες:
- Γνωριμία με τον HPV
- Γιατί ένα εμβόλιο; Το μέγεθος των προβλημάτων που προκαλεί ο HPV
- Τα τρία διαθέσιμα εμβόλια κατά του HPV
- Χρονοδιάγραμμα εμβολιασμού
- Αποτελεσματικότητα του εμβολίου HPV
- Ασφάλεια του εμβολίου κατά του HPV
- Αμφισβήτηση της ασφάλειας του εμβολίου: σημαντικότερα γεγονότα
- Άλλα αμφιλεγόμενα θέματα
- Αναπάντητα ερωτήματα …
- Συμπέρασμα
1. Γνωριμία με τον HPV

Ο HPV (ιός των ανθρωπίνου θηλώματος) είναι ένας ιός και μεταδίδεται από άτομο σε άτομο μέσω στενής επαφής δέρμα-με-δέρμα.
• Η HPV λοίμωξη είναι εξαιρετικά συνηθισμένη, και τις περισσότερες φορές το ανοσοποιητικό σύστημα θα καταφέρει να απαλλαχθεί από τον ιό.
• Από τους πάνω από 120 τύπους του ιού HPV, περίπου 12 υπότυποι (κυρίως οι 6 και 11) μπορεί να προκαλέσουν κονδυλώματα των γεννητικών οργάνων. Αυτοί οι λεγόμενοι τύποι “χαμηλού κινδύνου” μπορεί επίσης να προκαλέσουν μια σπάνια πάθηση που ονομάζεται υποτροπιάζουσα θηλωμάτωση του αναπνευστικού, στην οποία αναπτύσσονται κονδυλώματα στο λαιμό.
• Περίπου 15 τύποι του HPV (κυρίως οι τύποι 16 και 18) συνδέονται με τον καρκίνο. Ο καρκίνος του τραχήλου της μήτρας είναι η πιο συχνή μορφή καρκίνου που σχετίζεται με τον HPV, αλλά ο ιός μπορεί να προκαλέσει και άλλους καρκίνους: του αιδοίου, του κόλπου, του πρωκτού και του στοματοφάρυγγα (στόμα και το λαιμό), καθώς και καρκίνο του πέους στους άνδρες.
Μπορείτε να μάθετε περισσότερες πληροφορίες σχετικά με τον HPV εδώ.
2. Γιατί ένα εμβόλιο; Το μέγεθος των προβλημάτων που προκαλεί ο HPV

Τα κάτωθι στοιχεία θα σας δώσουν μία ιδέα της διάστασης των προβλημάτων που σχετίζονται με τον HPV:
-Παγκοσμίως, πάνω από 500.000 νέες περιπτώσεις καρκίνου του τραχήλου διαγιγνώσκονται ετησίως. Ο καρκίνος του τραχήλου της μήτρας είναι ο 4ος συχνότερος γυναικείος καρκίνος, και είναι η 2η πιο συνηθισμένη μορφή καρκίνου στις γυναίκες ηλικίας 15 έως 44 ετών (1).
Στις Ηνωμένες Πολιτείες, εκτιμάται ότι κάθε χρόνο υπάρχουν περίπου 26.000 νέα κρούσματα καρκίνων που οφείλονται σε HPV, από τα οποία 17.000 είναι γυναίκες και 9.000 άνδρες (2).
Στην Ευρώπη, περίπου 58.000 νέες περιπτώσεις καρκίνων που σχετίζονται με HPV εκτιμάται ότι θα εμφανιστούν κάθε έτος (3).
-Όσο αφορά της προκαρκινικές αλλοιώσεις, η εκτιμώμενη ετήσια επιβάρυνση κυμαίνεται μεταξύ 280.000 και 550.000 νέες περιπτώσεις ετησίως στην Ευρώπη (4).
-Εκτός από καρκίνους και προκαρκινικές αλλοιώσεις, το πρόβλημα των κονδυλωμάτων πρέπει επίσης να λαμβάνεται υπόψη. Τα κονδυλώματα είναι πολύ συνηθισμένα: 1 στα 10 άτομα θα έχουν κονδυλώματα κάποια στιγμή στη ζωή τους (5). Περίπου 800.000 νέες περιπτώσεις κονδυλωμάτων εκτιμάται ότι θα διαγνωστούν σε γυναίκες και άνδρες στην Ευρώπη (4). Αν και δεν είναι απειλητικά για τη ζωή, το κόστος που προκύπτει από την θεραπεία τους και η ψυχολογική επιβάρυνση που προκαλούν δεν πρέπει να παραμεληθόυν.
3.Τα τρία διαθέσιμα εμβόλια κατά του HPV

Από το 2006, 2 εμβόλια έχουν κυκλοφόρησει: Ένα διδύναμο (Cervarix), έναντι των τύπων HPV 16 και 18, που ευθύνονται για περίπου 70% των καρκίνων του τραχήλου και άλλων καρκίνων, και το άλλο τετραδύναμο (Gardasil® , ή Silgard® σε διάφορες χώρες) που περιέχει 4 τύπους του HPV: 16 και 18, σε συνδυασμό με HPV 6 και 11, που είναι υπεύθυνοι για περισσότερο από το 90% των κονδυλωμάτων.
Τον Δεκέμβριο του 2014, η αμερικανική Υπηρεσία Τροφίμων και Φαρμάκων (FDA) ενέκρινε ένα εμβόλιο εννέα-δύναμο, το Gardasil 9® (6), το οποίο, εκτός από τα 4 στελέχη που περιέχονται στο Gardasil (δηλαδή 6,11,16,18), συμπεριλαμβάνει τους τύπους 31, 33, 45, 52, και 58, υπεύθυνοι για ένα επιπλέον 20% καρκίνων που σχετίζονται με τον HPV (4). Το Gardasil 9 έχει πρόσφατα εγκριθεί και στην Ευρώπη (7).
4. Χρονοδιάγραμμα εμβολιασμού

Κάτωθι θα βρείτε ένα απόσπασμα από το “Πρόγραμμα Εμβολιασμών Παιδιών & Εφήβων 2015” από την Εθνική Επιτροπή Εμβολιασμών σχετικά με το εμβόλιο κατά του HPV:
- Στη χώρα μας διατίθενται το διδύναμο (HPV2) και το τετραδύναμο (HPV4) εμβόλιο HPV.
- Μικρότερη ηλικία χορήγησης: 9 έτη.
- Τα εμβόλια HPV2 και HPV4 χορηγούνται σε 2 δόσεις με μεσοδιάστημα 6 μηνών (σχήμα 0, 6) σε κορίτσια ηλικίας 11 έως 15 ετών.
- Εφόσον η έναρξη του εμβολιασμού γίνει μετά τη συμπλήρωση του 15ου έτους, χορηγούνται 3 δόσεις εμβολίου (σχήμα 0, 1-2, 6 μήνες).
- Σε περίπτωση που οι 2 δόσεις γίνουν σε μεσοδιάστημα μικρότερο των 6 μηνών απαιτείται και 3η δόση μετά τους 6 μήνες.
- Η μέγιστη προστασία επιτυγχάνεται εφόσον ο εμβολιασμός ολοκληρωθεί πριν την έναρξη της σεξουαλικής δραστηριότητας.
Στο σχετικό “Πρόγραμμα Εμβολιασμών Ενηλίκων 2015” αναφέρεται:
- Το εμβόλιο HPV συνιστάται στις γυναίκες 18-26 ετών (τρείς δόσεις) και θα χορηγείται δωρεάν μέχρι 31/12/2016.
- Τα HPV εμβόλια δεν συνιστώνται σε έγκυες γυναίκες. Ωστόσο, δεν είναι απαραίτητο να γίνεται τεστ εγκυμοσύνης πριν από την έναρξη του εμβολιασμού. Εάν διαπιστωθεί ότι μια γυναίκα είναι έγκυος μετά την έναρξη του εμβολιασμού, δεν συνιστάται διακοπή της κύησης και οι υπόλοιπες δόσεις συμπληρώνονται μετά την ολοκλήρωση της κύησης.
- Tο εμβόλιο χορηγείται δωρεάν και στους ομοφυλόφιλους άνδρες κάτω των 26 ετών (βλέπε παρακάτω “Εμβολιασμός στα αγόρια”).

Άλλες επισημάνσεις:
- Σε άλλες χώρες, όπως ΗΠΑ και Αυστραλία, τα αγόρια έχουν ενταχθεί στο πρόγραμμα εμβολιασμού με το ίδιο χρονοδιάγραμμα που ισχύει για τα κορίτσια (8, 9, 10).
- Εκτός του ότι τα εμβόλια είναι πιο αποτελεσματικά πριν από την έναρξη της σεξουαλικής δραστηριότητας, ο εμβολιασμός σε νεαρή ηλικία (πριν τα 14 έτη) έχει ως αποτέλεσμα υψηλότερη ανοσολογική απόκριση (8).
- Παρόλα αυτά, ο εμβολιασμός συνιστάται ανεξάρτητα από τη σεξουαλική δραστηριότητα ή από γνωστή λοίμωξη από τον HPV. Σε σεξουαλικά ενεργά άτομα, κάποιο όφελος αναμένεται να επιτευχθεί, επειδή είναι πολύ απίθανη η μόλυνση με όλους τους τύπους του HPV που περιλαμβάνονται στο εμβόλιο. Δεν συνιστάται να γίνει εξέταση για τον HPV πριν από τον εμβολιασμό.
- Τα εμβόλια είναι προληπτικά, δηλαδή, δεν εμποδίζουν την πρόοδο μιας προϋπάρχουσας μόλυνσης από τον ιό, και δεν θα θεραπεύσουν κάποια πάθηση που σχετίζεται με τον ιό (2).
- Φαίνεται να υπάρχει πρόσθετη προστασία από το εμβόλιο σε γυναίκες μέχρι την ηλικία των 45 ετών, όπως έδειξαν ορισμένες μελέτες (11). Ωστόσο, δεν υπάρχει σύσταση για εμβολιασμό σε άτομα ηλικίας 26 σε 45.
- Για το Gardasil 9 ισχύει το ίδιο σχήμα του Gardasil (0, 2 και 6 μήνες). Επαναληπτικός εμβολιασμός με το εμβόλιο εννέα-δύναμο δεν συνιστάται σε άτομα που προηγουμένως ολοκλήρωσαν τη σειρά τριών δόσεων με το εμβόλιο διδύναμο ή τετραδύναμο (8).
5. Αποτελεσματικότητα του εμβολίου HPV

Ο απώτερος σκοπός του εμβολιασμού κατά του HPV είναι η μείωση εμφάνισης των καρκίνων που σχετίζονται με τον ιό. Για προφανείς λόγους ηθικής, οι μελέτες που έγιναν για να αξιολογηθεί η αποτελεσματικότητα του εμβολίου όρισαν σταν τελικό σημείο (endpoint) τις προκαρκινικές βλάβες, δηλαδή CIN 2 και 3 (αλλοιώσεις του τραχήλου της μήτρας με δυνατότητα να εξελιχθούν σε καρκίνο). Άλλα τελικά σημεία αποτελεσματικότητας που αξιολογήθηκαν ήταν η επίπτωση της λοίμωξης από HPV και η επίπτωση των κονδυλωμάτων.
Μελέτες που διεξήχθησαν πριν την κυκλοφορία των εμβολίων έδειξαν ότι και τα δύο εμβόλια είχαν ένα υψηλό επίπεδο προστασίας για τους τύπους του HPV που περιέχονται στα εμβόλια: 98 έως 100% προστασία σε γυναίκες που δεν είχαν μολυνθεί με τους ιούς 16 ή 18 πριν τον εμβολιασμό, αν και η προστασία έναντι των προκαρκινικών βλαβών ήταν 30-40% στο σύνολο του εμβολιασμένου πληθυσμού (στον οποίο περιλαμβάνονταν γυναίκες που δεν είχαν ολοκληρώσει το σχήμα εμβολιασμού, ή που είχαν ήδη μολυνθεί με τον HPV πριν από τον εμβολιασμό) ( 12, 13, 14, 15). Διαπιστώθηκε επίσης διασταυρούμενη προστασία για άλλους τύπους του HPV (όπως τους 45 και 31), η οποία ήταν πιο ισχυρή με το Cervarix (16).
 Η επίδραση του εμβολιασμού στο γενικό πληθυσμό έχει επίσης αναλυθεί σε μερικές μελέτες. Η Αυστραλία ήταν η πρώτη χώρα να εισάγει ένα οργανωμένο πρόγραμμα εμβολιασμού κατά του HPV, και έχει πετύχει ένα από τα υψηλότερα ποσοστά συμμόρφωσης στον εμβολιασμό παγκοσμίως. Από το 2007 που ξεκίνησε το Εθνικό Πρόγραμμα Εμβολιασμού με το τετραδύναμο εμβόλιο, οι λοιμώξεις από τους τύπους του HPV που περιλαμβάνονται στο εμβόλιο μειώθηκαν από 29% σε 7% (17). Παρατηρήθηκε επίσης μείωση 93% στη διάγνωση γεννητικών κονδυλωμάτων (18). Επιπλέον, άλλες μελέτες έδειξαν μείωση σχεδόν 50% των προκαρκινικών βλαβών τραχήλου σε γυναίκες που είχαν λάβει όλες τις απαιτούμενες δόσεις του εμβολίου (19).
Η επίδραση του εμβολιασμού στο γενικό πληθυσμό έχει επίσης αναλυθεί σε μερικές μελέτες. Η Αυστραλία ήταν η πρώτη χώρα να εισάγει ένα οργανωμένο πρόγραμμα εμβολιασμού κατά του HPV, και έχει πετύχει ένα από τα υψηλότερα ποσοστά συμμόρφωσης στον εμβολιασμό παγκοσμίως. Από το 2007 που ξεκίνησε το Εθνικό Πρόγραμμα Εμβολιασμού με το τετραδύναμο εμβόλιο, οι λοιμώξεις από τους τύπους του HPV που περιλαμβάνονται στο εμβόλιο μειώθηκαν από 29% σε 7% (17). Παρατηρήθηκε επίσης μείωση 93% στη διάγνωση γεννητικών κονδυλωμάτων (18). Επιπλέον, άλλες μελέτες έδειξαν μείωση σχεδόν 50% των προκαρκινικών βλαβών τραχήλου σε γυναίκες που είχαν λάβει όλες τις απαιτούμενες δόσεις του εμβολίου (19).
Η Δανία έχει επίσης ένα οργανωμένο πρόγραμμα εμβολιασμού. Έξι χρόνια μετά την έναρξη του προγράμματος με το τετραδύναμο εμβόλιο, παρατηρήθηκε μείωση των προκαρκινικών βλαβών του τραχήλου της μήτρας, η οποία έφτασε στα 80% στις νεότερες ηλικίες (20).
Πρόσφατα, πραγματοποιήθηκε μια μελέτη με σκοπό να αξιολογηθεί η αποτελεσματικότητα του εννεα-δύναμου εμβολίου. Το Gardasil 9 μείωσε κατά 97% τις προκαρκινικές αλλοιώσεις του τραχήλου της μήτρας, του αιδοίου και του κόλπου που προκαλούνται από τις πέντε νέους τύπους HPV (HPV31/33/45/52/58) (21). Το εμβόλιο εννέα-δύναμο προκάλεσε επίσης ανοσολογική απάντηση κατά τους τύπους HPV 6 /11/16/18, η οποία ήταν εξίσου καλή ή καλύτερη από το τετραδύναμο εμβόλιο. (4, 22)
6. Ασφάλεια του εμβολίου κατά του HPV
Πολλές μελέτες έχουν αξιολογήσει την ασφάλεια των εμβολίων έναντι του HPV, τόσο πριν την κυκλοφορία τους όσο και μετά, οι οποίες δεν έδειξαν διαφορές στις παρενέργειες σε σύγκριση με ομάδες ελέγχου, ανεξάρτητα από ηλικία ή εθνικότητα (23).

Σύμφωνα με το CDC, οι πιο συχνές αναφερόμενες ανεπιθύμητες ενέργειες των εμβολίων είναι:
- Πόνος, ερυθρότητα ή πρήξιμο στο χέρι όπου έγινε το εμβόλιο
- Πυρετός
- Πονοκέφαλος ή αίσθημα κόπωσης
- Ναυτία
- Μυϊκοί πόνοι ή αρθραλγίες
Η λιποθυμία (επίσης γνωστή ως συγκοπή) και άλλα συνοδευόμενα συμπτώματα (όπως σπασμωδικές κινήσεις) δεν είναι ασυνήθιστη (24), ιδιαίτερα σε εφήβους.
Για το λόγο αυτό, συνιστάται όσοι λαμβάνουν το εμβόλιο να καθίσουν ή να ξαπλώσουν κατά τη διάρκεια του εμβολιασμού, και να μένουν καθιστοί για 15 λεπτά αφού έγινε (23).
Λαμβάνοντας υπόψη την ηλικία στην οποία πραγματώνεται ο εμβολιασμός (η οποία περιλαμβάνει και γυναίκες σε αναπαραγωγική ηλικία), ιδιαίτερη προσοχή έχει δοθεί στην έκβαση της εγκυμοσύνης. Καμία αύξηση σε ποσοστά αποβολών δεν έχει αναφερθεί για κανένα από τα εμβόλια (25). Επιπλέον, οι έγκυες γυναίκες που έχουν καταγραφεί δεν έχουν αυξημένο ποσοστό συγγενών ανωμαλιών (26, 27, 24).
Άλλες μελέτες έχουν επιβεβαιώσει την αποτελεσματικότητα και την ασφάλεια των εμβολίων στους άνδρες, τόσο στους ετεροφυλόφιλους όσο και στους άνδρες που κάνουν σεξ με άνδρες (28).
Οι σοβαρές παρενέργειες είναι πολύ σπάνιες (λιγότερο από 0,5%) (29), από τις οποίες οι πιο συχνές είναι επίμονη κεφαλαλγία, υπέρταση, γαστρεντερίτιδα, βρογχόσπασμος και αναφυλαξία. Η αναφερόμενη συχνότητά τους είναι παρόμοια με εκείνη των άλλων υποχρεωτικών εμβολίων (30).

Ορισμένες παρενέργειες έχουν προκαλέσει ανησυχία από τότε που εισήχθη το εμβόλιο, κυρίως τα αυτοάνοσα νοσήματα (ΑΝ) (όπως υποθυρεοειδισμός, ρευματοειδής αρθρίτιδα, σύνδρομο του Behcet, νόσος του Raynaud, διαβήτη τύπου 1 και λεύκη), οι νευρολογικές διαταραχές (π.χ. επιληψία, παράλυση, σύνδρομο Guillain-Barre, κεντρική απομυελίνωση και σκλήρυνση κατά πλάκας) και η φλεβική θρομβοεμβολή (ένας θρόμβος αίματος που φράζει μία φλέβα). Θα πρέπει να αναφερθεί ότι τα ΑΝ δεν είναι σπάνια σε εφήβους και νέους, ιδιαίτερα στις γυναίκες. Ως εκ τούτου, δεν είναι πάντα εύκολο να διαχωρίσουμε αιτιώδη από χρονική συσχέτιση. Μια πρόσφατη μελέτη συγκέντρωσε τα αποτελέσματα 9 μεγάλων μελετών (εκ των οποίων η μία ήταν μια ανασκόπηση 42 μελετών μαζί) προκειμένου να διερευνηθούν οι σοβαρές ανεπιθύμητες αντιδράσεις του εμβολίου κατά του HPV. Σε καμία από όλες αυτές τις μελέτες δεν βρέθηκαν ενδείξεις για αυξημένο κίνδυνο αυτοάνοσης ασθένειας, νευρολογικής διαταραχής, ή φλεβικής θρομβοεμβολής (31).
Η Παγκόσμια Συμβουλευτική Επιτροπή για την ασφάλεια των εμβολίων (GACVS), που ιδρύθηκε από τον Παγκόσμιο Οργανισμό Υγείας (WHO) παρέχει ανεξάρτητες, αυστηρά επιστημονικές συμβουλές για θέματα ασφαλείας των εμβολίων. Τον Δεκέμβριο του 2013 προέβηκε σε λεπτομερή ανασκόπηση όλων των διαθέσιμων στοιχείων σχετικά με την ασφάλεια των εμβολίων κατά του HPV, και κατέληξε στο συμπέρασμα ότι και τα δύο εμπορικά διαθέσιμα εμβόλια είναι ασφαλή (32). Παρομοίως, η Διεθνής Ομοσπονδία Μαιευτικής και Γυναικολογίας (FIGO), η Επιτροπή Γυναικολογικής Ογκολογίας και η Υποεπιτροπή για την πρόληψη του καρκίνου του τραχήλου της μήτρας υποστηρίζουν τη συνέχιση της χορήγησης των εμβολίων κατά του HPV στους κατάλληλους πληθυσμούς (33).
7. Αμφισβήτηση της ασφάλειας του εμβολίου: σημαντικότερα γεγονότα

Παρότι ορισμένες μεμονωμένες περιπτώσεις παρενεργειών είχαν περιγραφεί στο Ηνωμένο Βασίλειο και στην Αυστραλία (34), η Ιαπωνία ήταν η πρώτη χώρα στην οποία παρατηρήθηκε ότι, μετά τον εμβολιασμό, μερικά κορίτσια υπέφεραν από εντονότατους πόνους και αναπηρία. Τα εν λόγω περιστατικά είχαν μεγάλη δημοσιότητα σε εφημερίδες, τηλεοπτικές εκπομπές και social media, αλλά ανησύχησαν και την ιατρική κοινότητα. Ιάπωνες γιατροί δημοσίευσαν αργότερα μια σειρά από 44 κορίτσια που είχαν διαγνωστεί με το λεγόμενο Πολύπλοκο Περιοχικό Σύνδρομο Πόνου (complex regional pain syndrome ,CRPS) (35).
Λόγω αυτών των ανησυχιών, τον Ιούνιο του 2013, το Ιαπωνικό Υπουργείο Υγείας, Εργασίας και Πρόνοιας (MHLW) αποφάσισε να αναστείλει την ενεργή σύσταση για εμβολιασμό κατά του HPV. Η απόφαση αυτή δημιούργησε έντονη διαμάχη μεταξύ επιστημόνων και στην κοινή γνώμη, η οποία συνεχίζεται μέχρι και σήμερα (34).
Τον Μάρτιο του 2015, το τηλεοπτικό κανάλι της Δανίας TV2 προέβαλε ένα ντοκιμαντέρ με τίτλο: Τα εμβολιασμένα κορίτσια – άρρωστα και προδομένα. Οι δημοσιογράφοι συγκέντρωσαν περίπου 60 κορίτσια από όλη την Δανία που αρρώστησαν λίγο μετά τον εμβολιασμό κατά του HPV. Μεταξύ των γιατρών που εμφανίζονται στο ντοκιμαντέρ είναι η Louise Brinth, η οποία εξέτασε προσωπικά περίπου 80 κορίτσια με παρόμοια συμπτώματα. Η Δρ Brinth ανέφερε ότι τα κορίτσια παρουσιάζουν ζάλη, λιποθυμία, και έντονους πονοκεφάλους. Συγκεκριμένα είπε, “Έχουν κοιλιακό άλγος και ναυτία. Έχουν παράξενες μυϊκές κινήσεις που δεν μπορούν να ελέγξουν. Και νιώθουν εξαντλημένα… Βλέπουμε ένα μοτίβο που κραυγάζει στον ουρανό, και θα πρέπει να εξεταστεί από σοβαρή έρευνα”.

Τον Απρίλιο του 2015, η Δρ Brinth δημοσίευσε σε επιστημονικό περιοδικό για 53 ασθενείς που διαμαρτύρονταν για ορθοστατική δυσανεξία, σοβαρή κεφαλαλγία, υπερβολική κόπωση, γνωστική δυσλειτουργία, γαστρεντερικές ενοχλήσεις και διάχυτο πόνο. Οι περισσότερες από αυτές είχαν διαγνωστεί με μια σπάνια νόσο γνωστή ως Σύνδρομο ορθοστατικής ταχυκαρδίας (postural orthostatic tachycardia syndrome, POTS), και ήταν σε στενή χρονική συσχέτιση με το εμβόλιο κατά του HPV (36a, 36b).
To ντοκιμαντέρ της Δανίας είχε τεράστιο αντίκτυπο σε όλο τον κόσμο, τόσο στο ευρύ κοινό όσο και στην ιατρική κοινότητα. Μία κλειστή σελίδα στο Facebook που έχει συσταθεί για τα πιθανά θύματα των παρενεργειών του Gardasil στη Δανία τριπλασίασε τα -προσεκτικά ελεγχόμενα- μέλη της. Παρόμοιες ομάδες έχουν δημιουργηθεί στο Facebook και από άλλες χώρες.
Κατόπιν αιτήματος της Δανίας, ο Ευρωπαϊκός Οργανισμός Φαρμάκων (EMA) διεξάγει μια επανεξέταση της ασφάλειας των εμβολίων HPV. Ωστόσο, ο οργανισμός υπογραμμίζει ότι η αναθεώρηση αυτή “δεν αμφισβητεί ότι τα οφέλη των εμβολίων κατά του HPV υπερτερούν των κινδύνων τους”. Ο Οργανισμός επισημαίνει επίσης ότι, ενώ διεξάγεται η επανεξέταση, δεν συνιστάται καμία αλλαγή όσον αφορά τη χρήση των προϊόντων αυτών.

Τον Μάιο του 2015, η βρετανική εφημερίδα The Independent δημοσίευσε ένα άρθρο με τίτλο: Χιλιάδες έφηβες αρρώστησαν σοβαρά μετά το σχολικό εμβολιασμό ρουτίνας κατά του καρκίνου. Το άρθρο επικεντρώνεται στην ιστορία της Emily Ryalls, 17 ετών, η οποία άρχισε να αισθάνεται έντονους πόνους και δυσκολία στην αναπνοή αμέσως μετά το εμβόλιο κατά του HPV.
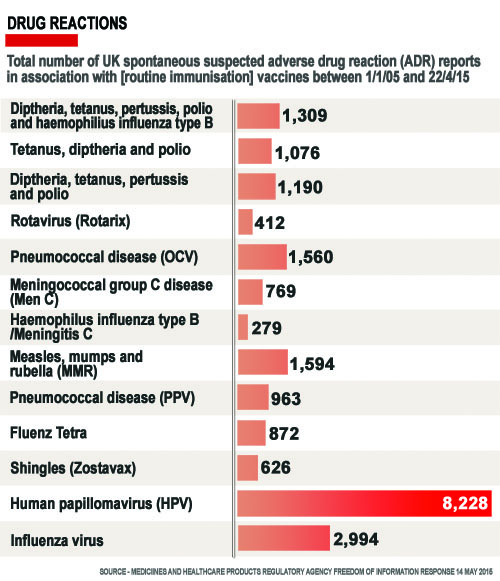
Η κα. Ryalls ανέφερε τα συμπτώματα της Emily στην Ρυθμιστική Αρχή Φαρμάκων και Προϊόντων Υγείας (MHRA), και δεν ήταν η μοναδική: οι ανεπιθύμητες ενέργειες μετά τον εμβολιασμό κατά του HPV αριθμούσαν 8.228, εκ των οποίων 2.587 είχαν χαρακτηριστεί ως “σοβαρές”, αρκετά περισσότερες από αυτές που αναφέρθηκαν μετά από άλλα υποχρεωτικά εμβόλια (βλέπε γράφημα). Η MHRA, όμως, αναφέρει ότι δεν υπάρχουν ανησυχίες σχετικά με τον αριθμό των ανεπιθύμητων ενεργειών που σχετίζονται με το εμβόλιο κατά του HPV και ότι τα «αναμενόμενα οφέλη στην πρόληψη ασθένειας και θανάτων από λοίμωξη HPV υπερτερούν των γνωστών κινδύνων”.
Η μητέρα της Emily, μαζί με άλλες 80 οικογένειες σε παρόμοια κατάσταση σε όλη τη Βρετανία ίδρυσαν τον Σύλλογο Κορών Θυμάτων του HPV Εμβολίου (Association for HPV Vaccine Injured Daughters (AHVID).
Όπως αναφέρθηκε από την εφημερίδα “Το σσυγκεκριμένο άρθρο προκάλεσε έντονη συζήτηση μεταξύ ιατρών, δημοσιογράφων και μελών του κοινού…».

Στη Γαλλία, η Εθνική Υπηρεσία Ασφάλειας των Φαρμάκων και Προϊόντων Υγείας (ANSM) δημοσίευσε πρόσφατα (το Σεπτέμβριο του 2015) τα αποτελέσματα της παρακολούθησης περισσότερων από 2 εκατομμύρια κορίτσια ηλικίας 13-16 ετών, εμβολιασμένα μεταξύ του 2008 και του 2013 για να αξιολογήσει την εμφάνιση παρενεργειών, κυρίως αυτοάνοσων νοσημάτων. Όταν ανέλυσε όλες τα νοσήματα μαζί, τα αποτελέσματά έδειξαν ότι δεν υπάρχει αυξημένο κίνδυνο εμφάνισης σοβαρών ανεπιθύμητων ενεργειών. Ωστόσο, όταν κάθε ασθένεια αναλύθηκε ξεχωριστά, παρατηρήθηκε μια τετραπλάσια αύξηση στην εμφάνιση του συνδρόμου Guillain Barré. Η μελέτη διαπίστωσε επίσης αυξημένο κίνδυνο φλεγμονώδους νόσου του εντέρου, αλλά η συσχέτιση ήταν αδύναμη.
Οι συγγραφείς καταλήγουν στο συμπέρασμα: “… τα αποτελέσματα της μελέτης αποδεικνύουν … καθησυχαστικά σχετικά με τον κίνδυνο αυτοάνοσης ασθένειας που σχετίζεται με τα εμβόλια HPV. Τα αναμενόμενα οφέλη από τον εμβόλιο αυτό, από την άποψη δημόσιας υγείας είναι πολύ μεγαλύτερα από τους ενδεχόμενους κινδύνους στους οποίους μπορεί να εκτίθενται τα κορίτσια” (37). Παρά αυτά τα «καθησυχαστικά» αποτελέσματα, το ποσοστό εμβολιασμού στη Γαλλία εξακολουθεί να είναι χαμηλό (κάτω του 30%).

Τον Σεπτέμβριο του 2015, μια άλλη δημοσίευση δίνει λεπτομερή στοιχεία για 45 άτομα από 13 χώρες, τα οποία ανέπτυξαν μια χρόνια πάθηση σύντομα μετά τη λήψη του εμβολίου κατά του HPV. “Ένα σύνδρομο με χρόνιο νευροπαθητικό πόνο, έντονη κόπωση, και βαθιά δυσλειτουργία του αυτονόμου νευρικού συστήματος μπορεί να εμφανιστεί μετά από εμβολιασμό HPV”, λένε οι συγγραφείς, με επικεφαλή τον Δρ. Manuel Martínez-Lavín, ειδικός σε παθήσεις χρόνιου πόνου από το Μεξικό. “Μετά από την πάροδο 4 ετών από τον εμβολιασμό, 93% των ατόμων “συνεχίζουν να έχουν συμπτώματα αναπηρίας και αδυνατούν να παρακολουθήσουν το σχολείο ή την εργασία τους” γράφουν οι συγγραφείς (38).
Το σύνδρομο POTS μετά από HPV εμβολιασμό έχει επίσης αναφερθεί στις Ηνωμένες Πολιτείες. Η Δρ Blitshteyn, νευρολόγος από τη Νέα Υόρκη, περιγράφει έξι περιπτώσεις ασθενών που ανέπτυξαν POTS μεταξύ 6 ημερών και 2 μηνών μετά τον εμβολιασμό HPV. Όλοι οι ασθενείς είχαν βελτίωση μετά από 3 χρόνια, αλλά κάποια υπολειμματικά συμπτώματα παρέμειναν (39).
Η Αμερικανική Υπηρεσία Τροφίμων και Φαρμάκων (FDA) και τα Κέντρα Ελέγχου και Πρόληψης Νοσημάτων (CDC), τόνισαν ότι ελεγχόμενες κλινικές δοκιμές σε δεκάδες χιλιάδες άτομα καθώς και η παρακολούθηση εκατομμυρίων ατόμων μετά την κυκλοφορία των εμβολίων δεν έχουν βρει καμία συσχέτιση του εμβολιασμού κατά του HPV με άτυπα σύνδρομα πόνου ή δυσλειτουργία του αυτόνομου συστήματος.

Η Δρ Diane Harper, μία Αμερικανίδα μαιευτήρας – γυναικολόγος, είναι μία από τους ειδικούς στον ιό HPV που κλήθηκαν να σχεδιάσουν τις κλινικές δοκιμές για το Gardasil και το Cervarix. Αν και αρχικά ήταν υπέρ του εμβολίου, τα τελευταία χρόνια έχει αμφισβητήσει την ασφάλεια του Gardasil. Έχει δηλώσει ότι “Το Gardasil έχει προκαλέσει τόσες σοβαρές ανεπιθύμητες ενέργειες όσο υπάρχουν θάνατοι από καρκίνο του τραχήλου της μήτρας κάθε χρόνου”. Εξάλλου, σε άρθρο που δημοσιεύθηκε τον Δεκέμβριο του 2009, κατέληξε στο συμπέρασμα ότι, λαμβάνοντας υπόψη τους περιορισμούς και τους κινδύνους των εμβολίων, τα οφέλη και οι κίνδυνοι του εμβολιασμού κατά του HPV θα πρέπει να συγκρίνονται με τα οφέλη και τους κινδύνους του προσυμπτωματικού ελέγχου του HPV (δηλαδή, το τεστ Παπανικολάου) για τη μείωση του καρκίνου του τραχήλου της μήτρας σε ένα οικονομικά αποδοτικό τρόπο (40).
Η Δρ Χάρπερ δεν υποστηρίζει τον υποχρεωτικό HPV εμβολιασμό στα σχολεία, γιατί πιστεύει πως η διάρκεια της προστασίας πιθανόν να είναι πολύ μικρή (βλέπε παρακάτω). Έχει επίσης κατακρίνει το σύντομο χρονικό διάστημα που τα εμβόλια δοκιμάστηκαν πριν την κυκλοφορία τους, και την παραπλανητική διαφήμιση των φαρμακευτικών εταιρειών. Μάθετε περισσότερα εδώ.
8. Άλλα αμφιλεγόμενα θέματα
Εμβολιασμός στα αγόρια

Η λογική του εμβολιασμού των αγοριών είναι να μειωθεί η μετάδοση του ιού HPV στα κορίτσια, και η προστασία τους από τους καρκίνους του στόματος και του πρωκτού (41). Δεδομένου ότι οι καρκίνοι αυτοί είναι πολύ σπάνιοι, έχει αμφισβητηθεί από ορισμένους επιστήμονες κατά πόσο αξίζει να εκτεθούν εκατομμύρια αγόρια στις πιθανές παρενέργειες του εμβολίου για να προστατευτούν τα κορίτσια, ή για την πρόληψη μιας τόσο σπάνιας μορφής καρκίνου (υπεύθυνος για μόλις 300 θανάτους στις ΗΠΑ), εάν το όφελος υπερτερεί τους κινδύνους και αν ο εμβολιασμός στους άνδρες είναι οικονομικά αποδοτικός. Ενώ χώρες όπως η Αυστραλία και οι ΗΠΑ περιλαμβάνουν τα αγόρια στις συστάσεις τους για εμβολιασμό, άλλες χώρες (πχ, το Ηνωμένο Βασίλειο και η Γαλλία) δεν έχουν ακόμη υιοθετήσει το μέτρο αυτό.
Οι άνδρες που κάνουν σεξ με άνδρες είναι μια ιδιαίτερη κατηγορία, δεδομένου ότι έχουν υψηλότερο κίνδυνο για καρκίνου του πρωκτού. Έτσι, μερικοί ειδικοί πιστεύουν πως σε αυτούς τους ανθρώπους (και όχι σε κάθε παιδί) θα πρέπει να προσφερθεί το εμβόλιο, και με αυτό το σκεπτικό στην Ελλάδα το εμβόλιο αποζημιώνεται δωρεάν στους ομοφυλόφιλους άνδρες κάτω των 26 ετών. Ωστόσο, το μέτρο αυτό μπορεί να είναι δύσκολο να εφαρμοστεί: για να καλύπτονται από το ταμείο τους, οι νέοι άνδρες υποχρεούνται να δηλώνουν (με μία υπεύθυνη δήλωση) τις σεξουαλικές τους προτιμήσεις.
Ανοσογονικότητα του Gardasil έναντι του Cervarix

Ανοσογονικότητα σημαίνει η ικανότητα του εμβολίου να προκαλέσει μια ανοσολογική απάντηση, με άλλα λόγια, η «δύναμη» του εμβολίου.
Οι περισσότερες χώρες υιοθέτησαν τον εμβολιασμό με Gardasil αντί του Cervarix υποθέτοντας ίση προστασία για τον καρκίνο, με την “μπόνους” προστασία για τα κονδυλώματα των γεννητικών οργάνων. Αλλά είναι πράγματι έτσι;
Αρκετές μελέτες έχουν δείξει ότι το Cervarix προκαλεί ισχυρότερη και μεγαλύτερης διάρκειας ανοσολογική απάντηση σε σχέση με το Gardasil (42, 43). Μάλιστα, αυτά τα εργαστηριακά ευρήματα έχουν επιβεβαιωθεί και από κλινικές μελέτες: με την πάροδο των χρόνων, η αποτελεσματικότητα του Cervarix για την προστασία από προκαρκινικές αλλοιώσεις (στην ομάδα που εμβολιάστηκε και δεν είχε εκτεθεί στον ιό προηγουμένως) ήταν 93%, ενώ στο Gardasil μειώθηκε στο 43% (44).
Ηλικία εμβολιασμού

Το θέμα αυτό έχει επίσης εγείρει έντονη συζήτηση και ανησυχία. Όπως αναφέρθηκε παραπάνω, η ανοσολογική απάντηση που προκαλείται από τα εμβόλια μπορεί να είναι περιορισμένης διάρκειας, ειδικά για το Gardasil. Αυτό μπορεί να αποτελεί ένα σοβαρό πρόβλημα, επειδή, όπως επισήμανε η Δρ Χάρπερ “… αν το HPV εμβόλιο δεν διαρκεί τουλάχιστον 15 χρόνια, ούτε ένας καρκίνος δεν πρόκειται ποτέ να προληφθεί, οι γυναίκες απλώς θα πάθουν καρκίνο αργότερα στη ζωή τους όταν η επίδραση του εμβολίου θα έχει φθαρεί“.
Αν αυτό το σύντομο χρονικό διάστημα προστασίας επιβεβαιώνεται από κλινικές μελέτες, μια αναμνηστική δόση θα λύσει αυτόν τον περιορισμό. Ωστόσο, θα αυξήσει σημαντικά το κόστος του εμβολίου, και επιπλέον, οι γυναίκες που δεν θα συμμορφώνονται με τη σύσταση αυτή, θα καθιστούν απροστάτευτες με την πάροδο του χρόνου.
Αύξηση της ελευθεριότητας;
Πολλοί άνθρωποι φοβούνται ότι το εμβόλιο κατά του HPV θα μπορούσε να θεωρηθεί από τα κορίτσια ως μια “άδεια” να έχουν σεξουαλικές επαφές χωρίς προστασία. Αυτό ερευνήθηκε από ορισμένες μελέτες, και έχουν αποδείξει πως δεν είναι αλήθεια: δεν παρατηρήθηκε καμία αύξηση στα σεξουαλικώς μεταδιδόμενα νοσήματα μεταξύ των εμβολιασμένων κοριτσιών (45), το ότι υποδηλώνει ότι ο εμβολιασμός είναι απίθανο να προωθήσει μη ασφαλή σεξουαλική δραστηριότητα.
9. Αναπάντητα ερωτήματα…

- Θα καταφέρει το εμβόλιο κατά του HPV να μειώσει τους θανάτους από καρκίνο του τραχήλου της μήτρας σε πραγματικές συνθήκες;
- Λόγω των προσφάτων γεγονότων, θα έπρεπε να σταματήσει η χορήγηση του εμβολίου μέχρι να ξεκαθαρίσει η κατάσταση;
- Αυτές οι τελευταίες ανησυχίες θα οδηγήσουν περισσότερες γυναίκες και κορίτσια να μην εμβολιαστούν, χάνοντας συνεπώς την ευκαιρία να προστατευτούν από την απειλή του καρκίνου;
- Δεδομένου ότι τα σύνδρομα που πιθανώς σχετίζονται με τα εμβόλια είναι δύσκολο να διαγνωστούν, είναι πιθανό να μην έχουν αναγνωριστεί στο παρελθόν; Μήπως για τον ίδιο λόγο θα γίνουν υπερβολικές αναφορές στο μέλλον;
- Μπορεί το εμβόλιο να δημιουργήσει μια ψευδή αίσθηση πλήρους προστασίας στις γυναίκες, με αποτέλεσμα λιγότερες γυναίκες να υποβληθούν σε προσυμπτωματικό έλεγχο (τεστ Παπ);
- Μήπως το εμβόλιο μείωνει τους τύπους του HPV που περιλαμβάνονται στο εμβόλιο, αλλά προκαλεί μια αύξηση εκείνων που δεν περιλαμβάνονται στο εμβόλιο;
10. Συμπέρασμα

Είναι πράγματι συναρπαστικό να έχουμε ένα εμβόλιο κατά του καρκίνου. Έχοντας δει γυναίκες να πεθαίνουν από καρκίνο του τραχήλου της μήτρας, εύχομαι πραγματικά ο καρκίνος αυτός να εξαφανιστεί από την επιφάνεια της Γης. Πρέπει όμως να διασφαλίζουμε ότι, στη προσπάθεια εξάληψής του, δεν θα κάνουμε περισσότερο κακό παρά καλό .

Τα εμβόλια έχουν κάνει πολύ καλό στην ανθρωπότητα (φανταστείτε αν ακόμα θα είχαμε ευλογιά, ή πολιομυελίτιδα…). Είναι αλήθεια πως κάθε ιατρική πράξη μπορεί να προκαλέσει παρενέργειες, και σε αυτό συμπεριλαμβάνονται και τα εμβόλια. Συνεπώς πρέπει να γνωρίζουμε ακριβώς ποιους κίνδυνους ενέχουν τα εμβόλια, και αν τα οφέλη υπερτερούν των κινδύνων.
Έχω την πεπιοήθηση πως οι κυβερνήσεις, οι επιστημονικές εταιρείες και οι φαρμακευτικές εταιρείες κάνουν μια προσπάθεια να ενημερώσουν τον κόσμο με υπευθυνότητα και ειλικρίνεια, έτσι ώστε όλοι μας -νέοι, γονείς και γιατροί- να μην χάσουμε την εμπιστοσύνη μας στην πρόοδο της επιστήμης, και τα εμβόλια να μην αποτελούν αντικείμενο προβληματισμού όσον αφορά την αξιοπιστία τους.
Θα χρειαστούν 10 έως 20 χρόνια για να καταλάβουμε το πραγματικό όφελος του εμβολίου κατά του HPV. Εν τω μεταξύ, να θυμάστε ότι τα τεστ Παπ ποτέ δεν έχουν σκοτώσει άνθρωπο, αντίθετα, έχουν σώσει εκατομμύρια ζωές. Ως εκ τούτου, μην ξεχνάτε να κάνετε τακτικά το τεστ Παπανικολάου!
Βιβλιογραφία
- International Agency for Research on Cancer, World Health Organization. Globocan 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012
- CDC Grand Rounds: Reducing the Burden of HPV-Associated Cancer and Disease. Morbidity and Mortality Weekly Report (MMWR) January 31, 2014 / 63(04);69-72
- Human Papillomavirus and Related Diseases Report. hpvcentre.net March 20th, 2015
- Hartwig S, et al: Estimation of the epidemiological burden of HPV-related anogenital cancers, precancerous lesions, and genital warts in women and men in Europe: Potential additional benefit of a nine-valent second generation HPV vaccine compared to first generation HPV vaccines. Papillomavirus Research, In Press (Available online 16 June 2015)
- Patel H, et al: Systematic review of the incidence and prevalence of genital warts. BMC Infectious Diseases 2013, 13:39
- “FDA approves Gardasil 9 for prevention of certain cancers caused by five additional types of HPV” (press release). 10 December 2014.
- “Gardasil® 9: new HPV vaccine approved in the European Union. The European Commission grants marketing authorisation for the first 9-valent HPV vaccine” (press release) Sanofi Pasteur MSD, June 17, 2015.
- Human Papillomavirus Vaccination. The American College of Obstetricians and Gynecologists, Committee Opinion Number 641, September 2015
- Recommendations on the Use of Quadrivalent Human Papillomavirus Vaccine in Males — Advisory Committee on Immunization Practices (ACIP), 2011. Morbidity and Mortality Weekly Report (MMWR), December 23, 2011 / 60(50);1705-1708
- Markowitz L, et al: Quadrivalent Human Papillomavirus Vaccine Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity and Mortality Weekly Report (MMWR), March 23, 2007 / 56(RR02);1-24
- Castellsagué X, et al: HPV vaccination against cervical cancer in women above 25 years of age: key considerations and current perspectives. Gynecologic Oncology 115 (2009) S15–S23
- Villa L, et al: Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: a randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol 2005; 6: 271–78
- The FUTURE II Study Group: Quadrivalent Vaccine against Human Papillomavirus to Prevent High-Grade Cervical Lesions. N Engl J Med 2007;356:1915-27
- Paavonen J, et al: Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet, Vol 374, No. 9686, p301–314, 25 July 2009
- Lehtinen M, et al: Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol, Vol 13, No. 1, p89–99, January 2012
- Harper D: Prophylactic human papillomavirus vaccines to prevent cervical cancer: review of the Phase II and III trials. Therapy 2008, 5 (3), 313-324
- Tabrizi SN, et al: Fall in human papillomavirus prevalence following a national vaccination program. J Infect Dis. 2012; 206(11):1645-1651
- Mariani L, et al: Early direct and indirect impact of quadrivalent HPV (4HPV) vaccine on genital warts: a systematic review. Adv Ther, 32 (2015), pp. 10–30
- Crowe E, et al: Effectiveness of quadrivalent human papillomavirus vaccine for the prevention of cervical abnormalities: case-control study nested within a population based screening programme in Australia. BMJ 2014;348:g1458
- Baldur-Felskov B, et at: early impact of Human Papillomavirus Vaccination on cervical Neoplasia—Nationwide Follow-up ofYoung Danish Women. J Natl Cancer Inst (2014) 106(3): djt460 doi:10.1093/jnci/djt460
- Joura E, et al: A 9-Valent HPV Vaccine against Infection and Intraepithelial Neoplasia in Women. N Engl J Med 2015; 372:711-723
- Petrosky E, et al: Use of 9-Valent Human Papillomavirus (HPV) Vaccine: Updated HPV Vaccination Recommendations of the Advisory Committee on Immunization Practices. Morbidity and Mortality Weekly Report (MMWR), March 27, 2015 / 64(11);300-304
- Center for Disease Control and Prevention. Human Papillomavirus (HPV) Vaccine Safety. Updated September 28, 2015
- Slade BA, et al: Postlicensure safety surveillance for quadrivalent human papillomavirus recombinant vaccine. JAMA, 2009;302(7):750–757
- Wacholder S, et al: Risk of miscarriage with bivalent vaccine against human papillomavirus (HPV) types 16 and 18: pooled analysis of two randomised controlled trials. BMJ 2010;340:c712
- Garland SM, et al: Pregnancy and infant outcomes in the clinical trials of a human papillomavirus type 6/11/16/18 vaccine: a combined analysis of five randomized controlled trials. Obstet Gynecol 2009;114(6):1179–1188
- Dana A, Buchanan KM, Goss MA, et al. Pregnancy outcomes from the pregnancy registry of a human papillomavirus type 6/11/16/18 vaccine. Obstet Gynecol. 2009;114(6):1170–1178
- Moscicki A, et al: HPV in men: an update. J Low Genit Tract Dis. 2011 Jul; 15(3): 231–234
- Gonçalves AK, et al: Safety, tolerability and side effects of human papillomavirus vaccines: a systematic quantitative review. Braz J Infect Dis, Vol 18, Issue 6, Nov–Dec 2014, Pages 651–659
- Lu B, et al: Efficacy and safety of prophylactic vaccines against cervical HPV infection and diseases among women: a systematic review and meta-analysis. BMC Infect Dis. 2011;11:13
- De Vincenzo R, et al: Long-term efficacy and safety of human papillomavirus vaccination. International Journal of Women’s Health 2014:6 999–1010
- World Health Organization. Global Advisory Committee on Vaccine Safety, 11–12 December 2013: Human papillomavirus vaccines safety (HPV). Wkly Epidemiol Rec. 2014;89(7):58–60
- Denny L: Safety of HPV vaccination: a FIGO statement. Int J Gynaecol Obstet. 2013;123(3):187–188
- Wilson R, et al: HPV Vaccination in Japan. The Continuing Debate and Global Impacts. A Report of the CSIS Global Health Policy Center. April 2015
- Kinoshita T, et al: Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine. Intern Med 53: 2185-2200, 2014
- a: Brinth L, et al: Suspected side effects to the quadrivalent human papilloma vaccine. Dan Med J 2015;62(4):A5064 b: Brinth L, et al: Orthostatic intolerance and postural tachycardia syndrome as suspected adverse effects of vaccination against human papilloma virus. Vaccine, 2015 May 21;33(22):2602-5
- Vaccination contre les infections à HPV et risque de maladies auto-immunes : une étude Cnamts/ANSM rassurante – Point d’information 13/09/2015
- Martínez-Lavín M, et: HPV vaccination syndrome. A questionnaire-based study. Clinical Rheumatology pp 1-3. Online 10 September 2015
- Blitshteyn S. Postural tachycardia syndrome following human papillomavirus vaccination. Eur J Neurol, Vol 21, 1, 135–139, 2014
- Harper, D: Current prophylactic HPV vaccines and gynecologic premalignancies. Current Opinion in Obstetrics and Gynecology 2009, 21:457–464
- Giuliano A, et al: Efficacy of Quadrivalent HPV Vaccine against HPV Infection and Disease in Males. N Engl J Med 2011;364:401-11
- Einstein M, et al: Comparative immunogenicity and safety of human papillomavirus (HPV)- 16/18 vaccine and HPV-6/11/16/18 vaccine: follow-up from months 12-24 in a Phase III randomized study of healthy women aged 18-45 years. Human Vaccines, vol. 7, no. 12, pp. 1343–1358, 2011
- Barzon L, et al: Neutralizing and cross-neutralizing antibody titres induced by bivalent and quadrivalent human papillomavirus vaccines in the target population of organized vaccination programmes. Vaccine, vol. 32, no. 41, pp. 5357–5362, 2014
- Di Mario S, et al: Are the Two Human Papillomavirus Vaccines Really Similar? A Systematic Review of Available Evidence: Efficacy of the Two Vaccines against HPV. Journal of Immunology Research, Volume 2015 (2015), Article ID 435141, 13 pages
- Jena A, et al: Incidence of Sexually Transmitted Infections After Human Papillomavirus Vaccination Among Adolescent Females. JAMA Intern Med. 2015;175(4):617-623
Photo Credits
Intro: Getty images; 1: curecancer.org; 2: m2.behance.net; 3: (collage) wikimedia commons; 4: cityofchicago.org; nkytribune.com; 5: english.cri.cn; hpv.health.gov.au; 6: marketingmag.ca; scontent.cdninstagram.com; 7: Japan: wikimedia commons; Denmark: vaccineimpact.com; UK: independent.co.uk; France: science-et-vie.com; POTS: pinterest.com; Harper: initiativecitoyenne.be; 8: bphc.org; migueljara.files.wordpress.com; lh3.googleusercontent.com; 9: healthvermont.gov; 10: compasscayman.com; i.dailymail.co.uk

 1) Τι είναι ο κολπικός τοκετός μετά από καισαρική τομή (VBAC);
1) Τι είναι ο κολπικός τοκετός μετά από καισαρική τομή (VBAC);
 3) Είμαι καλή υποψήφια για VBAC;
3) Είμαι καλή υποψήφια για VBAC;
 6) Ποια είναι τα πλεονεκτήματα ενός VBAC;
6) Ποια είναι τα πλεονεκτήματα ενός VBAC;
 7) Ποιοι είναι οι κίνδυνοι ενός VBAC;
7) Ποιοι είναι οι κίνδυνοι ενός VBAC;
 9) Τι να περιμένω κατά τη διάρκεια ενός VBAC;
9) Τι να περιμένω κατά τη διάρκεια ενός VBAC;