In the Part 1 of Home birth: Smart choice or risky business? we analyzed the issues of personal satisfaction, maternal safety and baby’s risks. Part 2 dealt with hospital transfers, water birth and the situation in the Netherlands. Check out the last three reasons women choose home birth, and read the final conclusion to decide whether home birth is a clever or a dangerous option…
7) “Home birth is cheap”
 Home birth is cheaper… provided that no transfer is needed and nothing goes wrong
Home birth is cheaper… provided that no transfer is needed and nothing goes wrong
Cost-effectiveness is an important issue in every country with an organized health system. Countries like England or the Netherlands, where the National Health System (NHS) covers the cost of deliveries, have calculated that is cheaper that women deliver at home, avoiding a more expensive hospital admission. For example, the UK NHS “prices” home birth £1066 and birth at a hospital £1631. The economical factor is one of the reasons certain professional organizations support home labor, such as the Royal College of Obstetrics and Gynaecologists (RCOG) which states that: “home birth is the most cost-effective place for delivery”.
But this cost analysis has been challenged, as it does not take in consideration the high transport rates; in fact, a Dutch report calculates a general 3-fold increase of costs in patients transported during labor, when the costs of the midwife, the transport system, the obstetrician and the hospital are included. In addition, the costs derived from the maintenance of an adequate transport system (ambulances and trained staff) should not be neglected. Assuming increased neonatal risks, admissions to the neonatal intensive care unit, the lifetime costs of supporting neurologically disabled children and potentially increased professional liability costs resulting from a complicated home birth can potentially inflate the costs.
Indicative of these unexpected expenses is the article Home birth: What the hell was I thinking? A journalist from The Guardian went on a mission following a home birth. After managing to deliver her child at home, both the woman and her baby had a complication and needed to be transferred to a hospital. Since the baby and the mother were not allowed to be in the same ambulance, two ambulances were required…
Regarding the costs arising from a private home birth, the situation varies in different countries; in the USA home births are not covered by health insurances, and a couple is expected to pay $1500 to 4500 to the midwife. Hospital births can range from $3,296 to 37,227, although they are usually covered totally or partially by the insurance. Of note: a doctor gets paid about $2500-4000, same as a midwife. Ιn Europe, a couple is expected to pay about 2000-3000 €; recently the Italian newspaper La Stampa published the article Home birth: a 3000 € luxury that does not convince doctors.
8) “Birth is not a disease, it’s a natural thing. Mother nature can’t go wrong”
 Unassisted childbirth: don’t try this at home – or anywhere else
Unassisted childbirth: don’t try this at home – or anywhere else
Indeed, Mother nature is great. If you think about it, the whole process of labor and delivery seems to be so perfect, almost magical… But “natural” is not a synonym of “risk-free”. Sometimes Mother nature can play strange games. We may believe we have everything under control, but things may flip just in a second: think earthquakes, or tsunamis… Exactly the same thing applies to childbirth: even when someone seems to be “low risk”, disaster can strike without any warning …
“Childbirth is inherently dangerous,” writes in her blog Amy Tuteur, an American obstetrician gynecologist. “In every time, place and culture, it is one of the leading causes of death of young women. And the day of birth is the most dangerous day in the entire 18 years of childhood”. Finally, she adds: “Why does childbirth seem so safe? Because of modern obstetrics. Modern obstetrics has lowered the neonatal mortality rate 90 per cent and the maternal mortality rate 99 per cent over the past 100 years.”
The absolute confidence in a woman body’s ability to deliver is expressed by supporters of unassisted childbirth (UC), the “hard core” version of home birth, which, although practised already since the 70s, it has lately seen a resurgence. Also known as freebirth, DIY (do-it-yourself) birth, unhindered birth, or unassisted home birth, it refers to women that intentionally deliver without the assistance of a physician or midwife; they may be completely alone (“solo birth”) or assisted by a lay person, such as the spouse, family, friend, or a non-professional birth attendant. There are no data on safety of UC, except that coming from a religious group in Indiana (USA) that found a perinatal mortality rate 2,7 times higher, and a maternal mortality rate 97 times higher than the state average.
Among the most famous UC advocates is Janet Fraser who, ironically, lost her baby after five days of home labour; in spite of that she continues to advocate for freebirth. In fact, UC is not endorsed by any scientific organization, as it is considered too dangerous. According to André Lalonde, executive vice-president of the Society of Obstetricians and Gynaecologists of Canada (SOGC):“Freebirth is the equivalent of playing Russian roulette with your child”.
9) “I have the right to deliver wherever I want”
 A home birth oxymoron: right to privacy vs. social media exposure
A home birth oxymoron: right to privacy vs. social media exposure
This is a very complex issue with ethical and legal connotations, which has originated intense debate among experts. Even scientific organizations differ in their recommendations. For example, The American College of Obstetricians and Gynecologists, until recently opposed to home births, has decided to temper its position: “…hospitals and birthing centers are the safest setting for birth, but it respects the right of a woman to make a medically informed decision about delivery.” On the other side, the American College of Nurse-Midwives (ACNM) maintains that “every family has a right to experience child birth in an environment where human dignity, self-determination, and the family’s cultural context are respected” and that “every woman has a right to an informed choice regarding place of birth and access to safe home birth services”. Let’s analyze the ethical and legal aspects of home birth:
Ethical issues
These are some of the ethicals dilemmas related to home birth:
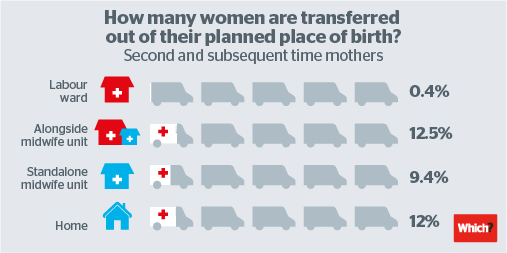
Mother vs child safety. Although hospital birth seems to increase maternal interventions in all studies (apparently without increasing severe risk), the baby’s safety remains a subject of debate; taking though in consideration all the studies, there seems to be increased risk for the baby. Let’s take for example the Birthplace study (which is in somewhere in the middle). This study found that, particularly for first time mothers, the baby’s risk is 3 times higher (of which more that half of the cases are death and brain damage). Is it ethically acceptable for a woman to value her birth experience over her baby’s welfare? Is maternal emotional wellbeing so important to justify risking the baby’s health?
Respect for dignity and privacy. “Dignity” may have a different meaning for each person. Some home births supporters feel that the presence of a doctor and the hospital staff make them feel “degraded”; moreover “for some women the possibility of the loss of privacy is a major issue, because privacy is a valued possession”.
Is it not contradictory that so many women, zealous advocates of home birth and their right to privacy, do not hesitate to publish their home birth photographs and videos -some of them with incredible details- in every social media site, where they are exposed to the eyes of millions of people?
Self-determination. In order to make truly informed decisions about childbirth options, women need to be informed of what they are and have the possibility to discuss them. Is it ethical to offer the option of home birth knowing that there is increased risk for her baby?
In theory, the person informing the pregnant woman should inform her objectively and avoid being paternalistic. The problem is that, informed decision-making implies accurate assessment of risks and benefits, but the safety of home birth remains debatable. Is it possible to inform objectively a pregnant woman about home birth? Or the information will be biased according to the health care provider beliefs or experiences?
Other possible ethical issues:
- In the home birth situation, are a woman’s reproductive rights and medical responsibility incompatible with each other?
- Where do a woman’s rights end and medical responsibility begins, especially considering that the physician is also responsible for the baby’s welfare?
- In case of a baby adverse outcome that could have been prevented in a hospital setting, what will be the psychological consequences for the couple?
- What is the psychological burden of a home birth in a family’s older children witnessing a home birth? What if a complication occur in their presence?
Legal issues
Legal issues can affect a woman’s decision to give birth at home in different countries. In certain places, home births are restricted, and even possibly criminally punishable, and family homes have been turned into crime scenes when women who have opted for homebirths experienced complications. In others countries, there are no regulating laws.
In Europe, the European Court of Human Rights (ECtHR) ruled in 2010 that Hungary had violated Article 8 of the European Convention on Human Rights (ECHR) because it had interfered with a woman’s right to choose where to give birth. Ms Ternovszky wanted to give birth at home but argued that she was prevented from doing so because a government decree dissuaded health care professionals from assisting home births. This case was the first decision by an international human rights organization on the right to choose the circumstances of giving birth, and was heralded by home birth advocates across Europe.
However, in a recent case against the Czech Republic, the Human rights judges decided that national authorities of each country has “considerable room for manoeuvre” when regulating home births, a matter for which there is no European consensus and which involves complex issues of health-care policy as well as allocation of State resources.
So, is home birth a smart choice or a risky business?
The Monty Python satirize the medicalisation of childbirth in The Meaning of Life
As an obstetrician who supports natural birth, I hear many times the women’s complaints about the excessive medicalization of childbirth. And I feel that sometimes they are right. However, being a mother myself, I never regretted my choice of a hospital birth for my children. After having helped so many women deliver their babies, I have seen many times complications that were totally unpredictable. Occasionally, these sudden complications are so serious, that we have to run -literally- from the delivery room to the operating room to save the baby or the mother! Therefore, even when having skilled professionals attending your home birth, even in countries with very organized structures, the distance to a hospital can prove fatal. Is for this reason that, in my opinion, a hospital birth is without any doubt the best choice for every woman. A birthing center attached to a hospital may also be a good choice.
True, the studies results are controversial, but for me “almost as safe as a hospital birth” is not enough to make me change my mind.
True also, a hospital birth is related to more epidurals, cesarean sections, instrumental deliveries and episiotomies. Regarding the epidural, if you can do it without one, that’s great! But sometimes labor pain is unbearable, and it’s not uncommon to see women without any pain relief who, when the moment to push comes, they are so exhausted and their pain is so overwhelming that they literally lose it. On the contrary, women with an epidural can be more focused and relaxed. The bottom line is: natural birth is not for everybody. And women don’t have to feel guilty because they chose to have an epidural. It’s better to have nice memories of your birth, and for that the epidural can help!
Whether too many cesareans sections are being done is a topic more controversial than home birth itself, and it would deserve a separate article. But what I can say is that, when cesarean sections are done in a judicious way by a conscious physician, they can save your life and your baby’s life. Since hospital births result in better neonatal outcome, it is clear to me that most interventions are an inevitable trade-off to save more babies or to avoid severe damage. The same goes for the controversial fetal monitoring, which may lead to more cesarean sections, it may not decrease perinatal mortality, but it reduces by 50% the risk of brain damage. Personally, I would do anything in my power to reduce the chances of having a brain damaged baby.
Of course, a lot that should be done -and can be done- to improve hospital birth: create home-like conditions to help women be relaxed and empowered, allow women to walk during labor, give them possibility to push and deliver in any position they wish, avoid unnecessary interventions such as systematic episiotomies, etc. I believe that some efforts are slowly being done worldwide, but we still have a long way to go!
In conclusion, a woman has the right to choose where to deliver; however, until the risks are clarified, maternal wellbeing may undermine the child’s welfare. Therefore, in my opinion, a natural hospital birth is the safest choice. Natural hospital birth IS possible! You just need motivation and a supportive team…
Hospitals should increase their efforts to provide women with a friendly environment so they can deliver their babies in comfort and total safety. Every baby is precious, every mother is precious!
Photo credits
7) screenterrier.blogspot.gr; 8) news.com.au; 9) vimeo.com, Wikimedia Commons, thebirthhour.com, Flickr.com, vimeo.com, homebirthaustralia.org, mindfulmamabirth.com, Flickr.com, huffingtonpost.co.uk, lifedaily.com